West Liberty Nursing and Rehabilitation is proud to spotlight resident Bonnie Dalton’s Success Story!
Bonnie came to West Liberty Nursing and Rehab Center on April 1st following compression fractures and complications. She began Occupational, Physical, and Speech therapy immediately upon arrival. Bonnie was an excellent patient, participating in all therapy tasks with a great attitude and strong work ethic. After lots of hard work, Bonnie was able to meet her goals and returned home just 20 days later! She was previously a nurse before the COVID-19 pandemic, and proudly boasts that she would love to come back and work at West Liberty Nursing and Rehab Center. Congratulations to Bonnie and her Care Team on their success!
CDC uses Travel Health Notices (THNs) to alert travelers and other audiences to health threats around the world and advise on how to protect themselves.
On April 18, 2022, CDC updated its COVID-19 THN system. Level 4 will no longer be based on COVID-19 incidence or case count alone. It will be reserved for special circumstances, such as rapidly escalating case trajectory or extremely high case counts, emergence of a new variant of concern, and healthcare infrastructure collapse. Levels 3, 2, and 1 will still be primarily determined by 28-day incidence or case counts as outlined below.
COVID-19 Travel Recommendations can be found in two places:
The 4-level system categorizes international destinations into the following levels:
Level 4: Special Circumstances / Do Not Travel
Do not travel to this destination.
If you must travel, make sure you are up to date with your COVID-19 vaccines before your trip.
Level 3: High Level Of COVID-19
Make sure you are up to date with your COVID-19 vaccines before traveling to this destination.
If you are not up to date with your vaccines, avoid travel to this destination.
If you have a weakened immune system or are more likely to get very sick from COVID-19, even if you are up to date with your COVID-19 vaccines, talk with your clinician about your risk and consider delaying travel to this destination.
Level 2: Moderate Level Of COVID-19
Make sure you are up to date with your COVID-19 vaccines before traveling to this destination.
If you have a weakened immune system or are more likely to get very sick from COVID-19, even if you are up to date with your COVID-19 vaccines, talk to your clinician about what additional precautions may be needed before, during, and after travel to this destination.
Level 1: Low Level of COVID-19
Make sure you are up to date with your COVID-19 vaccines before traveling to this destination.
Level Unknown: Unknown Level of COVID-19
Make sure you are up to date with your COVID-19 vaccines before traveling to this destination.
If you are not up to date with your vaccines, avoid travel to this destination.
If you have a weakened immune system or are more likely to get very sick from COVID-19, even if you are up to date with your COVID-19 vaccines, talk with your clinician about your risk, and consider delaying travel to this destination.
Level 4 will be reserved for special circumstances, such as rapidly escalating case trajectory or extremely high case counts, emergence of a new variant of concern, and healthcare infrastructure collapse. Other factors that may be considered include information such as vaccination rate and hospitalization rate. CDC works with country authorities through CDC country or regional offices to gather additional data as appropriate.
Level 1-3 Travel Health Notices are determined as follows:
Primary criteria for destinations with populations over 100,000
Incidence rate (cumulative new cases over the past 28 days per 100,000 population)
New case trajectory (Have daily new cases increased, decreased, or remained stable over the past 28 days?)
Primary criteria for destinations with populations of 100,000 or less
COVID-19 case counts* (cumulative new cases over past 28 days)
New case trajectory (Have daily new cases increased, decreased, or remained stable over the past 28 days?)
*CDC does not count identified imported cases (i.e., cases in travelers who were exposed in another country) against a destination’s total.
Secondary Criteria for Determining Travel Health Notice Levels
Reported case counts and incidence rates depend on testing capacity. CDC assesses testing capacity using two secondary criteria metrics: population testing rate and test-to-case ratio. The population testing rate is the number of tests conducted per 100,000 people over 28 days. The test-to-case ratio is the number of tests conducted for each case reported during the same 28-day period. Testing data are obtained from multiple sources, including Our World in Dataexternal icon, Foundation for Innovative Diagnosticsexternal icon, and country ministries of health.
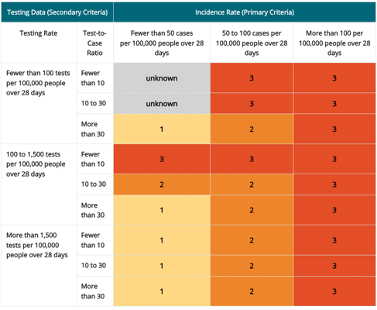
Travel Health Notice levels 1 through 3 for destinations with a population more than 100,000 people. Levels are based on combined 1) incidence rate (primary criteria) and 2) testing data (secondary criteria)
*Incidence rate is the primary criteria for destinations with a population more than 100,000 people. Testing data are the secondary criteria and that data includes both the testing rate (column 1) and test-to-case ratio (column 2). The resulting THN levels are shown in rows 3–11 of columns 3–5.
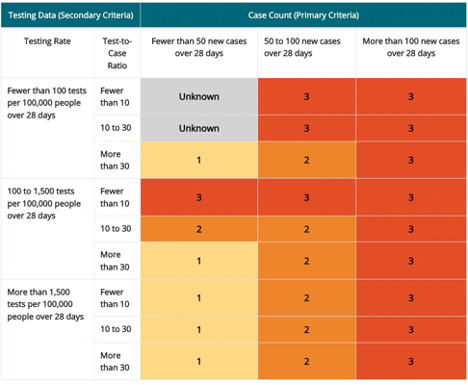
Travel Health Notice levels 1 through 3 for destinations with a population of 100,000 people or fewer. Levels are based on combined 1) case count (primary criteria) and 2) testing data (secondary criteria) *
*Case count is the primary criteria for destinations with a population fewer than or equal to 100,000 people. Testing data are the secondary criteria and that data includes both the testing rate (column 1) and test-to-case ratio (column 2). The resulting THN levels are shown in rows 3–11 of columns 3–5.
Population testing rates of more than 1,500 tests per 100,000 people over 28 days are considered sufficient to provide an accurate representation of COVID-19 in the destination. Rates less than or equal to 1,500 tests per 100,000 people over 28 days may signify concerns that testing is insufficient and may not provide an accurate representation of the incidence rate in the destination. The cutoffs for evaluating population testing ratesexternal icon have been adapted from the WHO guidelines.
The WHO determined a test-to-case ratio greater than or equal to 10 as the minimum indicator of sufficient surveillance capacity. A test-to-case ratio of less than 10 tests per case might indicate restrictive testing, or that only symptomatic people are being tested and undercounting the incidence rate (primary criteria). The preferred level is a test-to-case ratio of more than 30. The cutoffs for evaluating test-to-case ratios pdf icon[PDF – 18 pages]external icon have been adapted from the WHO guidelines.
When both the population testing rates and test-to-case ratios are high, CDC has confidence in a destination’s reported incidence. If either the population testing rate or test-to-case ratio is low, CDC has less confidence that the reported incidence accurately depicts the COVID-19 situation in the destination. In this situation, CDC adjusts a destination’s THN level as shown in the tables above. Countries with low incidence and testing rates are classified as unknown as well as countries that report data infrequently.
Level Unknown Travel Health Notices are determined as follows:
If a destination has insufficient data to make a THN level determination, its THN level is designated as “unknown”. Insufficient data means that the destination does not provide data or that the provided data are non-representative of the COVID-19 situation in the destination, making an accurate THN level determination difficult. This situation includes destinations with low COVID-19 incidence and low reported COVID-19 testing levels.
Raising a Travel Health Notice
CDC raises a destination’s THN level when the incidence rate (or case count) and testing metrics meet the THN threshold for a higher level and remain at that level for 14 consecutive days. The THN level may be raised before 14 days if there is a large increase in COVID-19 cases reported.
Lowering a Travel Health Notice
CDC lowers a destination’s THN level when the incidence rate (or case count) and testing metrics meet the THN threshold for a lower level and remain at that level for 28 consecutive days. Vaccination coverage rates and case trajectory will be considered when determining if the THN level can be lowered before 28 days.
Diagnostic testing is intended to identify current infection in individuals and should be performed on anyone that has signs and symptoms consistent with COVID-19 and/or following recent known or suspected exposure to SARS-CoV-2.
Examples of diagnostic testing include:
Testing anyone with symptoms consistent with COVID-19
Testing vaccinated and unvaccinated people who were exposed to someone with a confirmed or suspected case of COVID-19
Screening Testing
Screening tests are intended to identify people with COVID-19 who are asymptomatic and do not have known, suspected, or reported exposure to SARS-CoV-2. Screening helps to identify unknown cases so that measures can be taken to prevent further transmission.
Examples of screening include testing:
Employees in a workplace setting
Students, faculty, and staff in a school setting
A person before or after travel
Someone at home who does not have symptoms associated with COVID-19 and no known exposures to someone with COVID-19
Public Health Surveillance Testing
Public health surveillance is the ongoing, systematic collection, analysis, and interpretation of health-related data essential to the planning, implementation, and evaluation of public health practice. See CDC’s Introduction to Public Health Surveillance.
Public health surveillance testing is intended to monitor community- or population-level outbreaks of disease, or to characterize the incidence and prevalence of disease. Surveillance testing is performed on de-identified specimens, and thus, results are not linked to individual people. Public health surveillance testing results cannot be used for individual decision-making.
Public health surveillance testing may sample a certain percentage of a specific population to monitor for increasing or decreasing prevalence, or to determine the population effect from community interventions such as social distancing. An example of public health surveillance testing is when a state public health department develops a plan to randomly select and sample a percentage of all people in a city on a rolling basis to assess local infection rates and trends.
Regulatory Requirements for Diagnostic, Screening, and Public Health Surveillance Testing
Any laboratory or testing site that performs diagnostic or screening testing must have a Clinical Laboratory Improvement Amendments (CLIA) certificate and meet all applicable CLIA requirements. For more information, see the Centers for Medicare & Medicaid Services CLIA websiteexternal icon. Tests used for SARS-CoV-2 diagnostic or screening testing must have received an Emergency Use Authorization from the U.S. Food and Drug Administration (FDA) or be offered under the policies in FDA’s Policy for COVID-19 Testsexternal icon.
Tests used for SARS-CoV-2 public health surveillance on de-identified human specimens do not need to meet FDA and CLIA requirements for diagnostic and screening testing.
Reporting Diagnostic, Screening, and Public Health Surveillance Testing Results
Both diagnostic and screening testing results should be reported to the people whose specimens were tested and/or to their healthcare providers.
In addition, laboratories that perform diagnostic and screening testing must report positive diagnostic and screening test results to the local, state, tribal, or territory health department in accordance with Public Law 116-136, § 18115(a), the Coronavirus Aid, Relief, and Economic Security (CARES) Act. As of April 4, 2022, laboratories are no longer required to report negative results for non-NAAT tests (rapid or antigen test results). The Department of Health and Human Services published guidance on COVID-19 Pandemic Response, Laboratory Data Reporting: CARES Act Section 18115pdf iconexternal icon that specifies what data, in addition to test results, laboratories and testing sites should collect and electronically report.
Public health surveillance testing results cannot be reported directly to the people whose specimens have been tested and are not reported to their healthcare providers. Public health surveillance testing results (test results that are de-identified) can be reported in aggregate to local, state, tribal, or territory health departments upon request. Results from testing that is performed outside of a CLIA-certified facility or without an FDA-authorized test can only be reported to a health department if those results are used strictly for public health surveillance purposes, and not used for individual decision making.
Summary of Testing for COVID-19
Diagnostic
Screening
Public Health Surveillance
Symptomatic
Yes
No
N/A
Unvaccinated or vaccinated with known or suspected exposure
Yes
No
N/A
Unvaccinated and Asymptomatic without Known or Reported Suspected Exposure
No
Yes
N/A
Characterize Incidence and Prevalence in the Community
N/A
N/A
Yes
Testing of Personally Identifiable Specimens
Yes
Yes
No
Results may be Returned to Individuals
Yes
Yes
No
Results Returned in Aggregate to Requesting Institution
No
No
Yes
Results Reported to State Public Health Departments
Yes
Yes
If requested
Testing can be Performed in CLIA-Certified Laboratory
Yes
Yes
Yes
Testing can be Performed in a Non-CLIA-Certified Laboratory
No
No
Yes
Test System Must be FDA Authorized or be Offered under the Policies in FDA’s Guidance
To help prevent the spread of COVID-19 and help our country cope during the pandemic, CDC has occasionally issued legally binding orders and regulations.
People must wear face masks in indoor areas of public transportation traveling into, within, or out of the United States and indoors at U.S. transportation hubs, including airports.
Air passengers, 2 years or older, traveling to the United States from another country must present a negative COVID-19 test result or documentation of recovery from COVID-19 before boarding their flights. Regardless of vaccination status, passengers ages 2 or older are required to present a negative COVID-19 viral test result from a sample taken no more than 1 day before travel. Alternatively, passengers may present documentation showing that they tested positive for COVID-19 on a sample taken within the past 90 days and have been cleared to travel (documentation of recovery).
CDC issued an Order to implement the President’s direction on safe resumption of global travel during the COVID-19 pandemic and provided guidance to airlines, other aircraft operators, and passengers in Technical Instructions and Frequently Asked Questions.
All non-U.S.-citizen, non-immigrants, with limited exceptions, traveling to the United States by air must be fully vaccinated and show proof of vaccination.
CDC issued an Order on October 25, 2021 requiring airlines and other aircraft operators to collect contact information for passengers before they board a flight to the United States from a foreign country. The purpose of collecting this information is to identify and locate passengers who may have been exposed to a person with a communicable disease for public health follow-up. Airlines will retain the information for 30 days and transmit the information to CDC upon request for contact tracing and public health follow-up to keep people safe.
Following a public health determination, the CDC Director is terminating the Order under 42 U.S.C. §§ 265, 268 and 42 C.F.R. § 71.40 suspending the right to introduce certain persons into the United States. The implementation of the termination of the Order will be on May 23, 2022.
CDC considered multiple factors in its public health assessment and finds that, at this time, the available COVID-19 mitigation tools, as well as the fact that 97% of the U.S. population lives in a county identified as having “low” COVID-19 Community Level, will sufficiently mitigate the COVID-19 risk for U.S. communities and make an order under 42 U.S.C. §§ 265, 268 and 42 C.F.R. § 71.40 no longer necessary. This Termination will be implemented on May 23, 2022, to enable the Department of Homeland Security (DHS) to implement appropriate COVID-19 mitigation protocols, such as scaling up a program to provide COVID-19 vaccinations to migrants, and prepare for full resumption of regular migration processing under Title 8 authorities.
During the COVID-19 pandemic, CDC issued an order suspending the right to introduce certain noncitizens attempting to enter the U.S. from Canada or Mexico (regardless of country of origin) at or between ports of entry. CDC has terminated the Order with respect to unaccompanied noncitizen children.
On October 21, 2021, CDC Director Rochelle P. Walensky, M.D., M.P.H., endorsed the CDC Advisory Committee on Immunization Practices’ (ACIP) recommendation for a booster shot of COVID-19 vaccine in certain populations. The FDA’s authorization and CDC’s recommendation for use are important steps forward as we work to stay ahead of the virus and keep Americans safe.
For individuals who received a Pfizer-BioNTech or Moderna COVID-19 vaccine, the following groups are eligible for a booster shot at 6 months or more after their initial series:
65 years and older
Age 18+ who live in long-term care settings
Age 18+ who have underlying medical conditions
Age 18+ who work or live in high-risk settings
For the nearly 15 million people who got the Johnson & Johnson COVID-19 vaccine, booster shots are also recommended for those who are 18 and older and who were vaccinated two or more months ago.
There are now booster recommendations for all three available COVID-19 vaccines in the United States. Eligible individuals may choose which vaccine they receive as a booster dose. Some people may have a preference for the vaccine type that they originally received, and others may prefer to get a different booster. CDC’s recommendations now allow for this type of mix and match dosing for booster shots.
Millions of people are newly eligible to receive a booster shot and will benefit from additional protection. However, today’s action should not distract from the critical work of ensuring that unvaccinated people take the first step and get an initial COVID-19 vaccine. More than 65 million American remain unvaccinated, leaving themselves- and their children, families, loved ones, and communities- vulnerable.
Available data right now show that all three of the COVID-19 vaccines approved or authorized in the United States continue to be highly effective in reducing risk of severe disease, hospitalization, and death, even against the widely circulating Delta variant. Vaccination remains the best way to protect yourself and reduce the spread of the virus and help prevent new variants from emerging.
The following is attributable to Dr. Walensky:
“These recommendations are another example of our fundamental commitment to protect as many people as possible from COVID-19. The evidence shows that all three COVID-19 vaccines authorized in the United States are safe- as demonstrated by the over 400 million vaccine doses already given. An, they are all highly effective in reducing the risk of severe disease, hospitalization, and death, even in the midst of the widely circulating Delta variant.”
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.OK